All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know GvHD.
The GvHD Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the GvHD Hub cannot guarantee the accuracy of translated content. The GvHD Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The GVHD Hub is an independent medical education platform, sponsored by Medac and supported through independent educational grants from Incyte, Sanofi and Therakos. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View GvHD content recommended for you
 Hildegard Greinix
Hildegard GreinixDo you know... Which of the following statements is false regarding the rationale for the use of ECP in SR-aGvHD?
During the 52nd Annual Meeting of the EBMT, the GvHD Hub held a live symposium on March 24, 2026, titled “Focusing GvHD care through the eyes of providers and patients: Practical insights on ECP”. Here, we share a presentation by Hildegard Greinix, Vienna, AT, describing her clinical experience in treating graft-versus-host disease (GvHD) with extracorporeal photopheresis (ECP).
Symposium | Physician’s perspective: How I treat GvHD with ECP
Symposium | Physician’s perspective: How I treat GvHD with ECP
Greinix presents two patient case studies, providing practical insights into the use of ECP for the treatment of acute GvHD (aGvHD) and chronic GvHD (cGvHD). In both cases, she explains that ECP could be considered as a second-line or later treatment option, either as monotherapy or in combination with other agents, owing to its immunomodulatory mechanism of action and favorable safety profile. She also explores key considerations and patient factors that inform treatment selection and initiation.
Clinical case 1: aGvHD
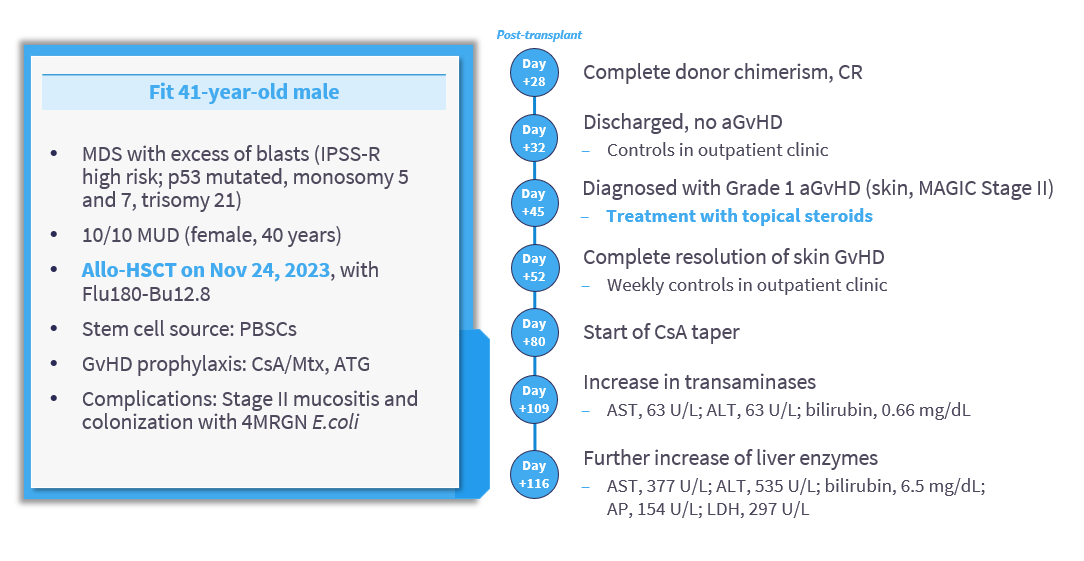
Greinix begins by presenting a clinical case of a fit 41-year-old male with myelodysplastic syndromes (MDS) who underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT). On Day 45 post-transplant, he developed Grade 1 aGvHD involving the skin (Mount Sinai Acute GvHD International Consortium [MAGIC] Stage III) (Figure 1). Initial management consisted of topical corticosteroids. As symptoms progressed, subsequent diagnostic work‑up confirmed Grade 3 steroid‑refractory (SR)-aGvHD involving the liver and lower gastrointestinal tract (MAGIC Stage III). ECP was initiated on Day 126 post-transplant and incorporated as part of third‑line therapy in combination with cyclosporin A, systemic corticosteroids, and ruxolitinib. This combined approach enabled successful steroid tapering and complete resolution of SR-aGvHD on Day 205 post-transplant. ECP therapy was discontinued on Day 235.
Figure 1. Clinical case of a 41-year-old male with aGvHD
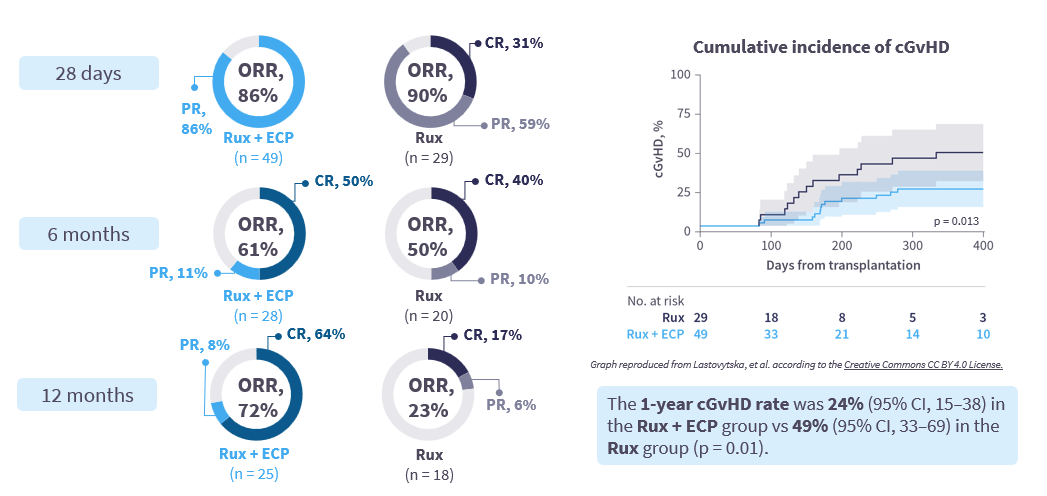
Greinix also considers data from clinical studies of ECP for the treatment of aGvHD, including a retrospective study of patients with SR-aGvHD treated with ruxolitinib + ECP or ruxolitinib alone (Figure 2).1
Figure 2. Retrospective study of patients with SR-aGvHD treated with ruxolitinib ± ECP during 2015–2022 (N = 78)1
Key takeaways:
- ECP can be considered as a second-line or later treatment option, alone or in combination with other agents, for patients with SR-aGvHD due to its immunomodulatory mechanism of action and favorable safety profile.2–4
- As ECP does not cause generalized immunosuppression,5–7 it may be used in patients with infections.
Clinical case 2: cGvHD
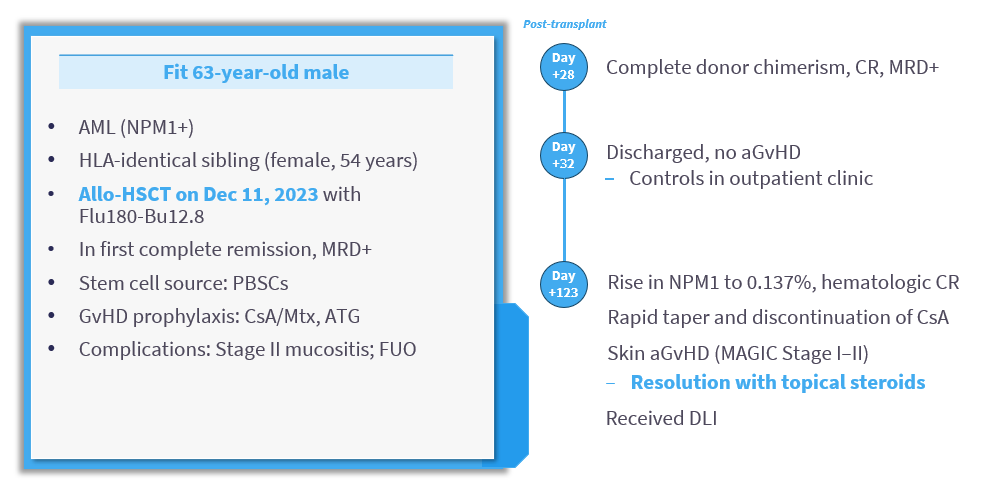
Greinix presents a second clinical case of a fit 63‑year‑old man with acute myeloid leukemia (AML) who underwent allo‑HSCT. On Day 123 post-transplant, he developed Grade 1 aGvHD with skin involvement (MAGIC Stage I–II) (Figure 3). aGvHD resolved with topical corticosteroids, after which the patient received three escalating doses of donor lymphocyte infusion (DLI). In July 2025, ECP was initiated in response to development of progressive sclerotic cGvHD, affecting the skin (National Institutes of Health [NIH] Stage III) and joints/fascia (NIH Stage II). Continuation of ECP enabled tapering of systemic corticosteroids and led to improvement in superficial sclerosis on the lower legs, while deep sclerosis of the ankles persisted (skin, NIH Stage III; joints/fascia, NIH Stage I). At the time of presentation, ECP was ongoing and administered over 2 consecutive days every 4 weeks.
Figure 3. Clinical case of a 63-year-old male with cGvHD
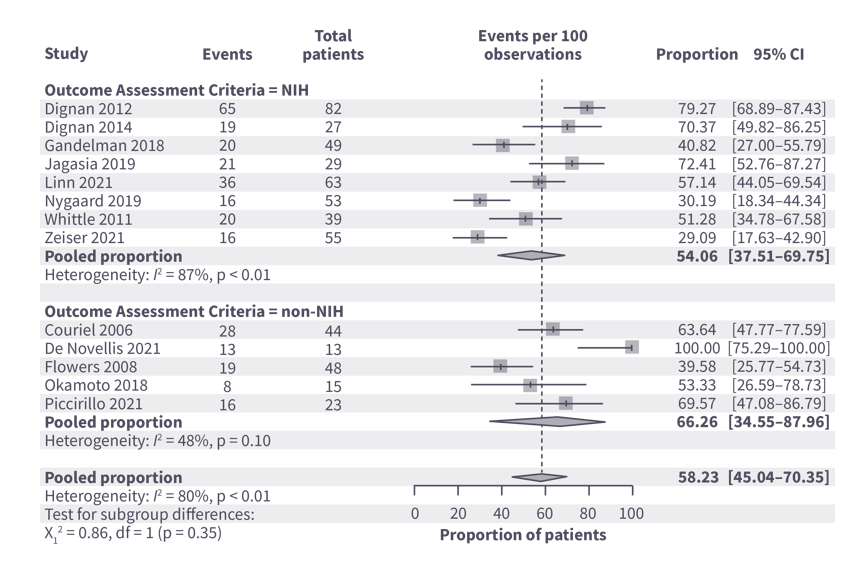
Greinix also considers data from studies of ECP for the treatment of cGvHD, including a meta-analysis of ECP in SR-cGvHD, showing improved response rates observed after a longer treatment duration (ORR, 45.3% at 3–4 months and 58.2% at 6–8 months) supporting the long-term clinical effectiveness of ECP (Figure 4).8
Figure 4. Meta-analysis of ECP in SR-cGvHD – ORR at 6–8 months*
Key takeaway:
ECP can be considered as a second-line or later treatment option, alone or in combination with other agents, for patients with SR-cGvHD, particularly those with sclerodermatous SR-cGvHD – a setting where ECP has demonstrated benefit.7,9
This educational activity is independently supported by Therakos. All content was developed by the faculty in collaboration with SES. Funders were allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:





