All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know GvHD.
The GvHD Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the GvHD Hub cannot guarantee the accuracy of translated content. The GvHD Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The GVHD Hub is an independent medical education platform, sponsored by Medac and supported through independent educational grants from Incyte, Sanofi and Therakos. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View GvHD content recommended for you
Symposium | Impact of clinical manifestations on treatment selection in SR-cGvHD
Featured:
 Corey Cutler
Corey CutlerDo you know... In the AGAVE-201 trial, which three organ systems demonstrated the highest response rates to axatilimab 0.3 mg?
During the 8th International Chronic Graft-versus-Host Disease Symposium, the GvHD Hub held a live symposium on May 22, 2026, titled Evolving treatment strategies in SR‑cGvHD: Optimizing patient selection across current and emerging therapies. Here, we share a presentation by Corey Cutler, Boston, US, discussing the impact of clinical manifestations on treatment selection in steroid-refractory chronic graft-versus-host disease (SR-cGvHD).
Symposium | Impact of clinical manifestations on treatment selection in SR-cGvHD
Symposium | Impact of clinical manifestations on treatment selection in SR-cGvHD
Cutler provides an overview of the inflammatory and fibrotic mechanisms underlying cGvHD, including the roles of the Janus kinase (JAK)1/2, Rho-associated kinase (ROCK)1/2, and colony-stimulating factor-1 receptor (CSF-1R) signaling pathways. He outlines the heterogeneous, organ-specific responses observed with targeted therapies and highlights that treatment selection may be informed by consideration of expected organ-specific responses and disease phenotype, with growing efforts to target the underlying biological mechanisms of cGvHD.
Key points
- Heterogeneous organ-specific responses have been observed with targeted therapies for cGvHD (Figure 1), highlighting the potential value of tailoring therapy according to distinct clinical manifestations.1–4
Figure 1A. Organ-specific responses with axatilimab*
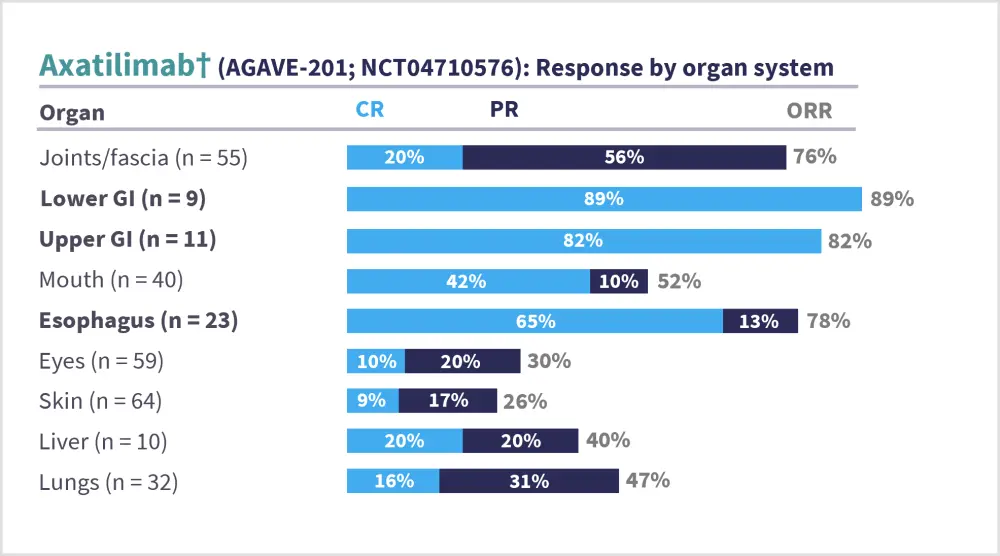
*Data from Wolff, et al.1
†0.3-mg dose group.
CR, complete response; GI, gastrointestinal; ORR, overall response rate; PR, partial response.
Figure 1B. Organ-specific responses with belumosudil*
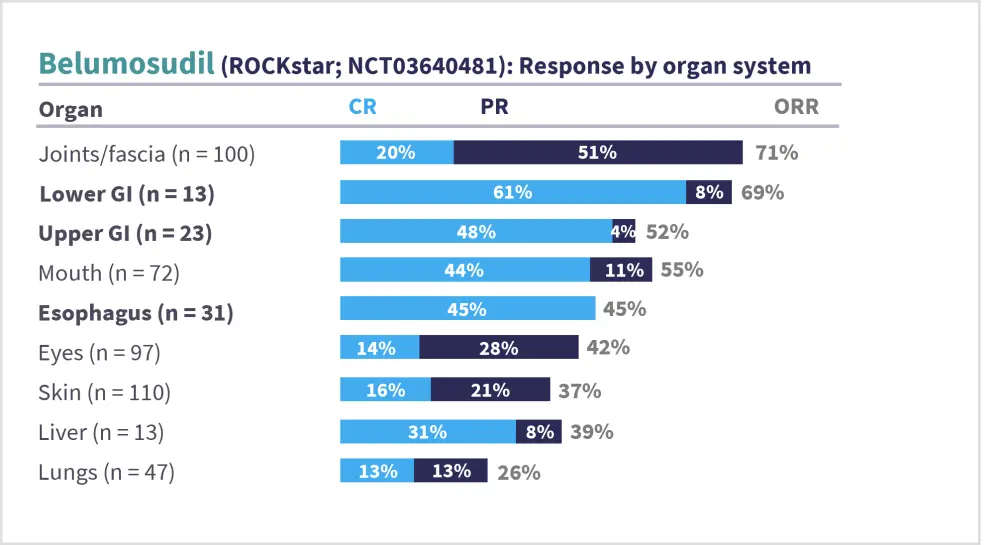
*Data from Cutler, et al.2
CR, complete response; GI, gastrointestinal; ORR, overall response rate; PR, partial response.
Figure 1C. Organ-specific responses with ruxolitinib*
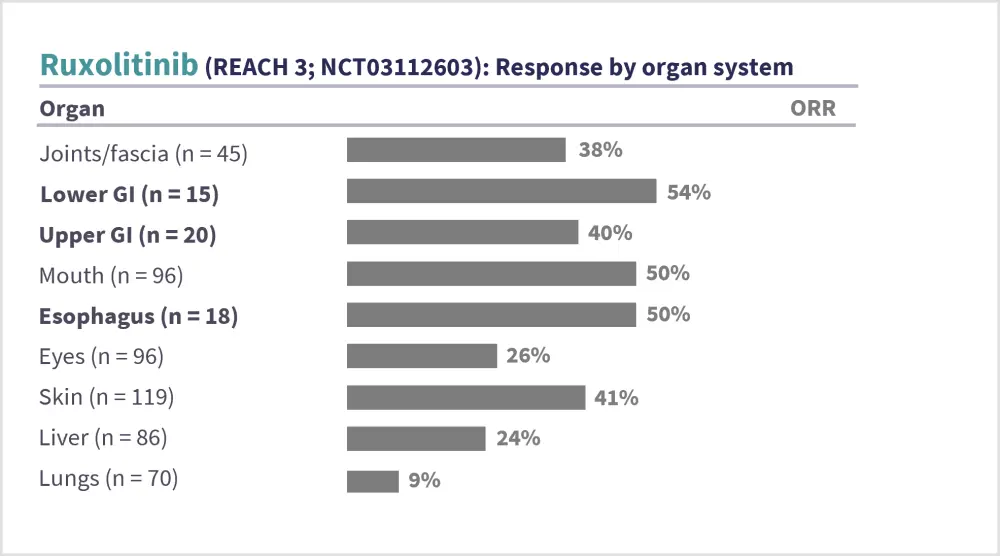
*Data from Zeiser, et al.3
GI, gastrointestinal; ORR, overall response rate.
Figure 1D. Organ-specific responses with rovadicitinib*
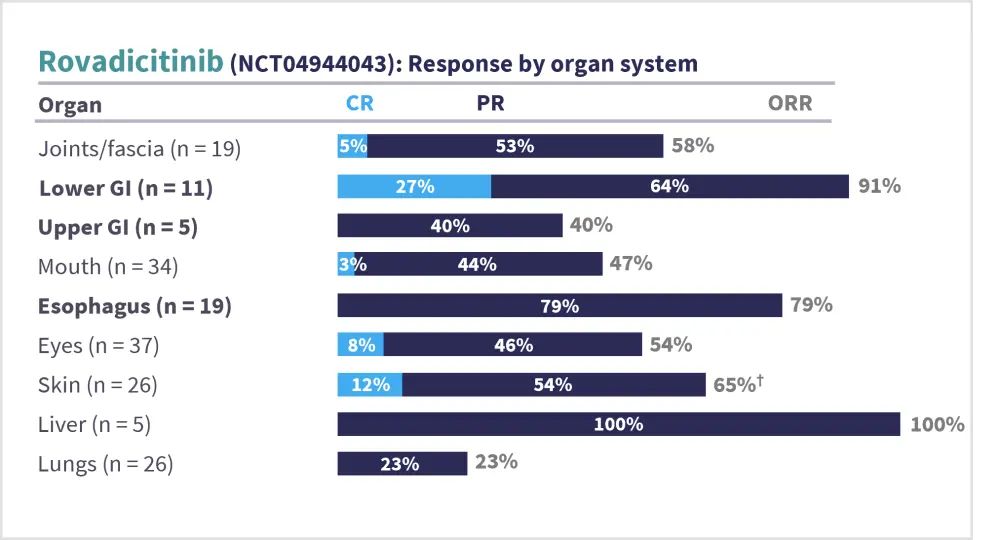
*Data from Zhao, et al.4
†The total ORR is reported as 65%, reflecting rounding of the CR and PR to the nearest decimal place.
CR, complete response; GI, gastrointestinal; ORR, overall response rate; PR, partial response.
- cGvHD arises from a cascade of immune dysregulation, disordered tissue repair, and progressive fibrosis, which can be broadly conceptualized into three phases: 1) tissue injury and early inflammation; 2) dysregulated B- and T-cell immunity; and 3) fibrosis.5–9
- Ibrutinib, axatilimab, belumosudil, and ruxolitinib are broadly approved for all manifestations of cGvHD; however, data for specific fibrotic complications are limited or absent from the respective registrational trials.10
- While these trials reported organ-specific involvement and responses, the nature of organ involvement was typically not specified. However, in the AGAVE‑201 trial, axatilimab was associated with reductions in sclerotic skin surface area, skin tightening, and symptoms related to skin thickening in patients with sclerotic skin manifestations.1,10
- Ruxolitinib, axatilimab, and belumosudil act through distinct mechanisms, inhibiting the JAK1/2, CSF-1R, and ROCK2 signaling pathways, respectively, and thereby modulating the inflammatory and/or fibrotic components of cGvHD.9,11–13
- The mechanisms of action of these agents have been previously described on the GvHD Hub.
- To enable clinical manifestations to meaningfully guide treatment selection in cGvHD, advances are needed in biomarkers pointing to organ-specific pathophysiology, understanding the mechanism of action of drugs, and organ-specific comparative trials.
- Pending these advances, treatment of fibrotic cGvHD is guided by several key goals:15,16
- Preventing further inflammation, thereby limiting subsequent fibrotic progression.
- Promoting fibrosis reversal by direct immunosuppressive mechanisms.
- In an analysis of tissue-level immune dynamics in 20 patients with oral cGvHD from the ROCKstar trial, ROCK2 inhibition was associated with reductions in type I and type II collagen in the oral buccal mucosa, as well as the number of T cells and interleukin-17-producing cells.13
- Facilitating fibrosis reversal by non-immunologic mechanisms.
- Several growth factors and their associated signaling pathways promote fibrosis by regulating fibroblast activation, epithelial cell apoptosis, epithelial-mesenchymal transition, and endothelial-mesenchymal transition; interfering with these pathways may target the molecular drivers of fibrosis and modify GvHD progression.17
- Fibrotic cGvHD is characterized by aberrant tissue repair and accumulation of myofibroblasts derived from multiple cellular lineages; targeting upstream cellular contributors to the myofibroblast pool may reduce or prevent fibrosis.18,19
- Several anti-fibrotic compounds are under development that target growth factors20–28
- Treatment selection may therefore be guided by expected organ-specific responses and disease phenotype, with a growing focus to address the underlying biological mechanisms of cGvHD.
This educational resource is independently supported by Sanofi. All content is developed by the faculty in collaboration with SES. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:

.webp&w=3840&q=75)

