All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know GvHD.
The GvHD Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the GvHD Hub cannot guarantee the accuracy of translated content. The GvHD Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The GVHD Hub is an independent medical education platform, sponsored by Medac and supported through independent educational grants from Incyte, Sanofi and Therakos. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View GvHD content recommended for you
 Daniel Wolff
Daniel WolffDo you know... Which of the following situations would indicate that a switch to third-line treatment for cGvHD should be considered?
During the 8th International Chronic Graft-versus-Host Disease Symposium, the GvHD Hub held a live symposium on May 22, 2026, titled “Evolving treatment strategies in SR‑cGvHD: Optimizing patient selection across current and emerging therapies”. Here, we share a presentation by Daniel Wolff, Regensburg, DE, outlining treatment options for steroid-refractory chronic graft-versus-host disease (SR-cGvHD).
Symposium | Current treatment options for SR-cGvHD
Symposium | Current treatment options for SR-cGvHD
Wolff reviews available therapeutic options for SR-cGvHD, including key data from pivotal trials of approved and widely adopted therapies. He discusses indications for transitioning to second- and third-line treatments, outlines his approach to managing SR-cGvHD, and highlights remaining unmet treatment needs.
Key points
- cGvHD is a major cause of late morbidity, occurring in 30–50% of patients who undergo allogenic hematopoietic stem cell transplantation.1–4
- Quality of life is significantly impaired in patients with cGvHD, and although corticosteroids remain the standard first-line treatment, long-term use is associated with significant toxicity.5–7
- Approximately 50% of patients with cGvHD become refractory to or dependent on steroids, and patients with SR-cGvHD have significantly increased morbidity and mortality. Therefore, there is a major unmet need for novel, steroid-sparing approaches to cGvHD treatment.6,7
- Several treatment options are approved for the management of SR-cGvHD (Figure 1), including ibrutinib (a Bruton’s tyrosine kinase inhibitor), belumosudil (a Rho-associated kinase 2 inhibitor), ruxolitinib (a Janus kinase 1/2 inhibitor), and axatilimab (a colony-stimulating factor receptor blocking monoclonal antibody), with data from several pivotal trials supporting their approval (Figure 2).6,8–15
Figure 1. Current treatment options for SR-cGvHD: Approval timeline*
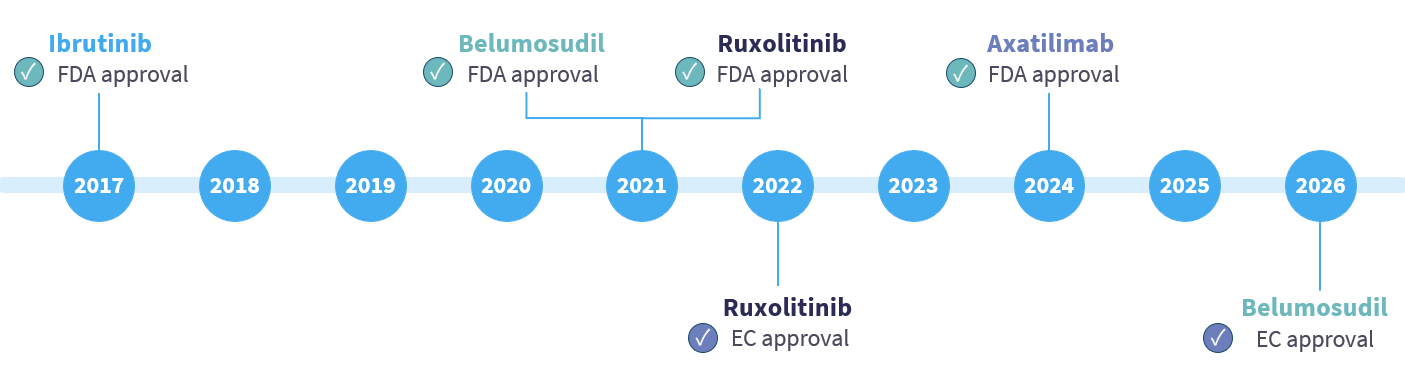
Figure 2. Summary of pivotal trials of approved therapies for SR-cGvHD*
- Although not approved, extracorporeal photophoresis (ECP) is a widely adopted therapy for SR-cGvHD.
- In a single-center study of patients with cGvHD treated with ECP (n = 87) or no ECP (n = 202), 6-month overall response rate was 76% in patients treated with ECP vs 68% in patients with no ECP. Response did not differ when ECP was used before, concomitant with, or after ruxolitinib and/or belumosudil.16
- Despite available treatment options, clinical outcomes in SR-cGvHD remain sub-optimal.
- Treatment effectiveness varies depending on the type of cGvHD manifestation and the affected organs (inflammatory [i.e., skin, liver] vs fibrotic [i.e., lung, skin]).6,17,18
- Real-world data suggest that fibrotic manifestations, including lung involvement, show lower responses to ruxolitinib and may therefore require alternative therapies.19,20
- Response to first-line steroid treatment can indicate whether second-line treatment should be considered (Figure 3).4,21
Figure 3. Indications for second-line treatment of SR-cGvHD*

- There are various factors that may arise during assessment of patients that signal a change of treatment could be required. Examples include increases in National Institute of Health (NIH) scores (skin, eyes, and oral), loss of photographic range of motion ≥1 or progression by NIH grade (fascia), or drop of forced expiratory volume in 1 second >10% in the absence of infection (lung). 4,21,22
- Response to second-line treatment can also indicate whether third-line treatment should be considered (Figure 4).4,21,23
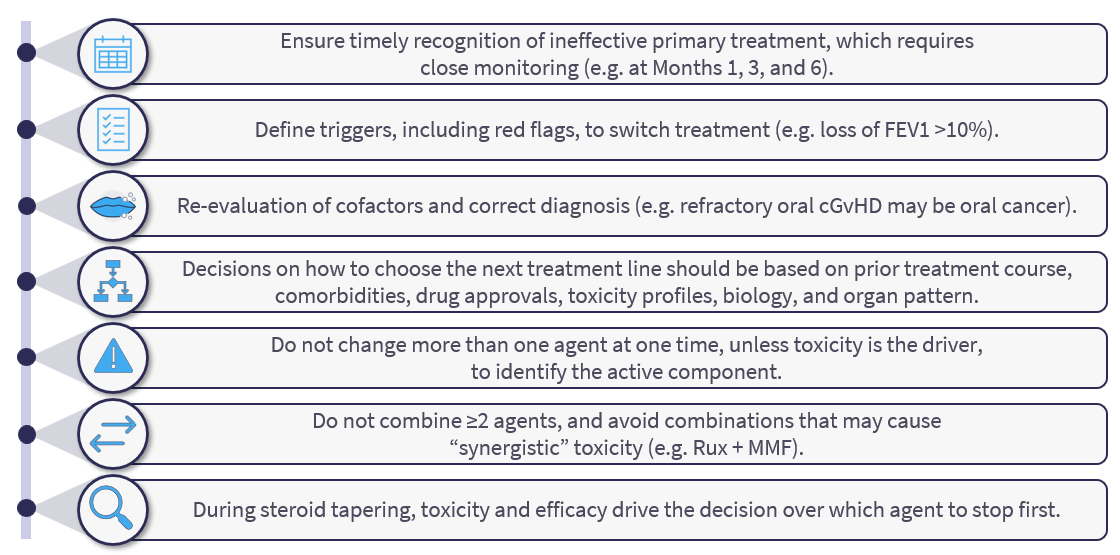
Figure 4. Indications for third-line treatment of SR-cGvHD*

- When proceeding with third-line treatment, it is recommended to avoid switching more than one drug at once (except in patients showing rapid progression), in order to facilitate identification of the effective agent.4
- Wolff provided a summary of his approach to treatment of SR-cGvHD (Figure 5).
Figure 5. Approach to treatment of SR-cGvHD
Ongoing unmet treatment needs
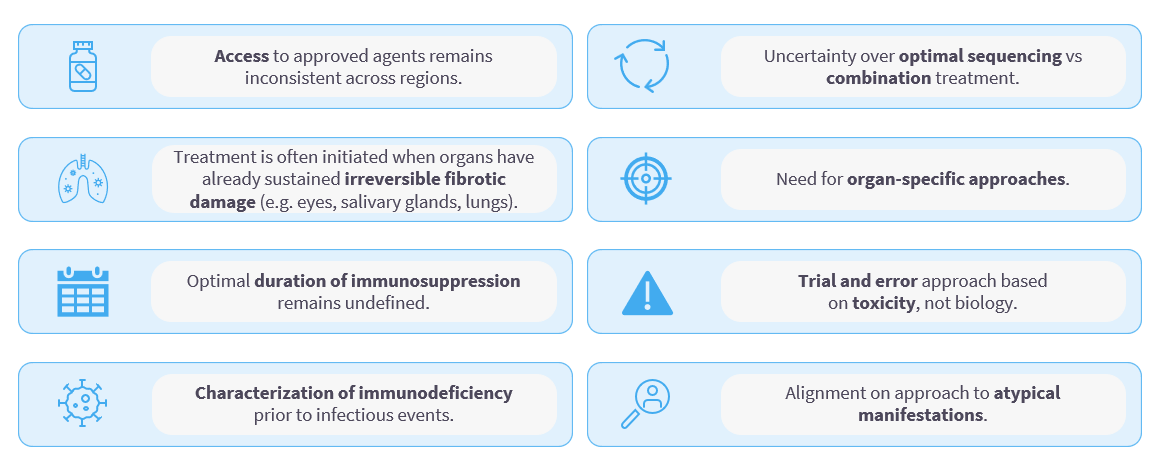
- Despite the investigation and approval of several steroid-sparing drugs in recent years, several unmet needs remain in the treatment of SR-cGvHD (Figure 6).4,24–28
Figure 6. Unmet needs in the treatment of SR-cGvHD*
This educational resource is independently supported by Sanofi. All content is developed by the faculty in collaboration with SES. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:

.webp&w=3840&q=75)

