All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know GvHD.
The GvHD Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the GvHD Hub cannot guarantee the accuracy of translated content. The GvHD Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The GVHD Hub is an independent medical education platform, sponsored by Medac and supported through independent educational grants from Incyte, Sanofi and Therakos. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View GvHD content recommended for you
 Zinaida Perić
Zinaida PerićDo you know... Which of the following statements best describes the therapeutic rationale for the use of rovadicitinib in SR-cGvHD?
During the 8th International Chronic Graft-versus-Host Disease Symposium, the GvHD Hub held a live symposium on May 22, 2026, titled Evolving treatment strategies in SR‑cGvHD: Optimizing patient selection across current and emerging therapies. Here, we share a presentation by Zinaida Perić, University of Rijeka, HR, outlining emerging treatment strategies for steroid-refractorychronic graft-versus-host disease (SR-cGvHD).
Symposium | Emerging treatment strategies for SR-cGvHD
Symposium | Emerging treatment strategies for SR-cGvHD
Perić highlights the growing shift toward targeted approaches that directly address the inflammation and fibrosis associated with cGvHD. She reviews the latest clinical data for several novel agents and combination approaches under evaluation for the treatment of SR-cGvHD, while emphasizing the need for larger-scale studies to confirm clinical benefit.
Key points
- Current therapies for SR-cGvHD demonstrate variable and often suboptimal efficacy, with reported response rates from 30% to 85%, highlighting the limitations of non-specific approaches.1
- Treatment is increasingly shifting toward targeted and better-tolerated approaches that directly address the inflammatory and fibrotic mechanisms underlying cGvHD while minimizing broad immunosuppression.1
- Belumosudil is approved by the U.S Food and Drug Administration (FDA) and received conditional marketing authorization from the European Commission in March 2026, expanding third-line treatment options for patients with SR-cGvHD.2,3
- Several emerging agents and combinations are under investigation for the treatment of SR-cGvHD (Table 1).4–13
Table 1: Mechanistic overview of emerging agents and combinations in SR-cGvHD*
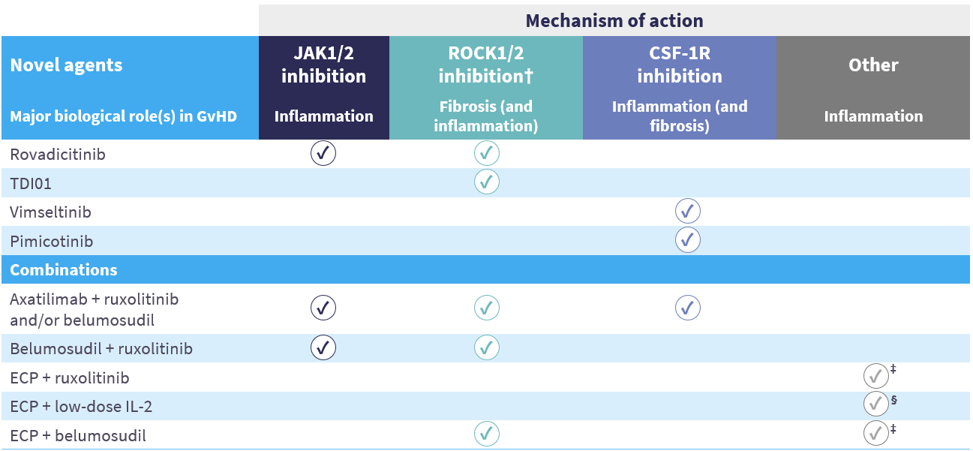
Emerging agents
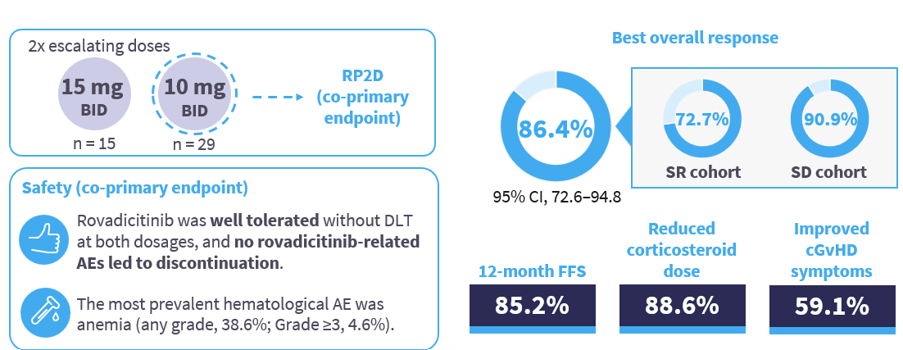
- Rovadicitinib (TQ05105) is a dual Janus kinase (JAK) 1/2 and Rho-associated kinase (ROCK) 1/2 inhibitor that has been evaluated in patients with moderate/severe SR or steroid-dependent (SD) cGvHD (N = 44) in a phase Ib/IIa study (NCT04944043; Figure 1).4
Figure 1: Key results from the phase Ib/IIa study evaluating rovadicitinib in SR or SD cGvHD*
- TDI01 is a second-generation ROCK2 inhibitor that has been evaluated in a phase Ib/II study (NCT06169722) in patients with moderate/severe cGvHD after one to five prior lines of therapy (LoT; N = 60).5
- The best overall response rate (ORR) was 75% in the 200 mg cohort and 86.2% in the 400 mg cohort.
- Grade ≥3 treatment-emergent adverse events (TEAEs) and treatment-related AEs were reported in 51.7% and 38.3% of patients, respectively.
- Vimseltinib is a novel colony-stimulating factor 1 receptor (CSF-1R) inhibitor approved by the FDA and European Medicines Agency for the treatment of adults with tenosynovial giant cell tumor.14,15
- Based on its manageable safety profile, vimseltinib is now being evaluated in a phase II study in patients with cGvHD (NCT06619561).6
- Pimicotinib, another CSF-1R inhibitor, has been evaluated in a phase II study (NCT06186804) in adults with cGvHD after ≥1 prior LoT (N = 28).7
- The 6-month ORR was 57.7% (66.7% in patients with moderate cGvHD; 52.9% in patients with severe cGvHD).
- TEAEs, Grade ≥3 TEAEs, and serious TEAEs occurred in 78.6%, 35.7%, and 21.4% of patients, respectively.
Combination approaches
- Given that inflammation and fibrosis often coexist in cGvHD, combining agents with complementary mechanisms of action may enable broader disease control, deeper responses, and reduced steroid exposure.11,16,17
- The combination of axatilimab + ruxolitinib and/or belumosudil has been evaluated in a retrospective, single-center study in patients with severe, treatment-refractory cGvHD (N = 8).17
- The ORR at any time was 25% per 2014 National Institute of Health consensus criteria and 75% per Clinically Significant Symptomatic Improvement as deemed by the provider.
- Three Grade 3 serious AEs (osteomyelitis, septic arthritis, and elevated gamma-glutamyl transferase level) occurred in a single patient.
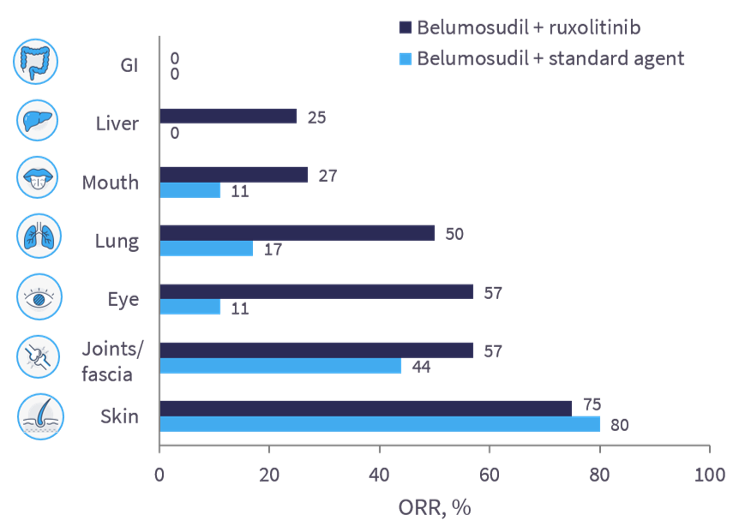
- Belumosudil + ruxolitinib has also been investigated in a retrospective, observational study in patients with SR-cGvHD (N = 26), reporting numerically higher mean ORR across most organ systems (except skin and gastrointestinal tract) compared with belumosudil + a standard agent (Figure 2).18
- Belumosudil + ruxolitinib appeared to be well tolerated without excess toxicity.
Figure 2: Organ-specific ORR in patients with SR-cGvHD receiving belumosudil in combination with ruxolitinib or a standard agent*
- Extracorporeal photopheresis (ECP) + ruxolitinib has been evaluated in patients with SR-cGvHD in a retrospective, single-center study (N = 23), showing a best response at any time of 74% (complete response, 9%; partial response, 65%).19
- Cytomegalovirus reaction and cytopenia occurred in 26% and 48% of patients, respectively.
- ECP in combination with low-dose interleukin-2 or belumosudil has also been investigated in patients with cGvHD.20,21
- Larger-scale studies are needed to confirm benefit and long-term outcomes of these emerging strategies in patients with SR-cGvHD.
This educational resource is independently supported by Sanofi. All content is developed by the faculty in collaboration with SES. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:

.webp&w=3840&q=75)

