All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know GvHD.
The GvHD Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the GvHD Hub cannot guarantee the accuracy of translated content. The GvHD Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The GVHD Hub is an independent medical education platform, sponsored by Medac and supported through independent educational grants from Incyte, Sanofi and Therakos. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View GvHD content recommended for you
Visual Abstract | Long-term outcomes with ruxolitinib + ECP in SR-aGvHD
Do you know... In a retrospective study by Lastovytska et al., what was the 12-month cGvHD rate in patients with SR-aGvHD treated with ruxolitinib + ECP?
Although allogeneic hematopoetic stem cell transplant is potentially curative for patients with hematological malignancies, the development of acute graft-versus-host disease (aGvHD) remains a major limitation.1 Glucocorticoids are the standard first-line treatment of aGvHD and chronic GvHD (cGvHD); however, not all patients respond to treatment.1
Ruxolitinib, a JAK1/2 inhibitor, is approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for patients with aGvHD and cGvHD.2–4 In the REACH2 trial (NCT02913261), in patients with aGvHD treated with ruxolitinib, overall response rates decreased from 62% at Day 28 to 40% at Day 56, suggesting long-term disease control remains an unmet need.1,5 Combination therapies are of clinical interest to address this, with initial studies underway. Extracorporeal photophoresis (ECP), a leukapheresis-based procedure, is an established treatment for steroid-refractory (SR-) GvHD, and, recently, Lastovytska et al. conducted a retrospective study to investigate the efficacy of ruxolitinib + ECP vs ruxolitinib alone in patients with SR-aGvHD treated between 2015 and 2022.1,6
Patients (N = 78) received oral ruxolitinib and steroid therapy followed by either ruxolitinib alone or ruxolitinib + ECP.1 Response rates at 6 and 12 months were higher with ruxolitinib + ECP than with ruxolitinib alone, suggesting improved long-term control of aGvHD. Furthermore, while there was no difference in 1-year non-relapse mortality and 2-year overall survival between treatment groups, a significant cGvHD relapse-free survival benefit was observed with ruxolitinib + ECP vs ruxolitinib alone.
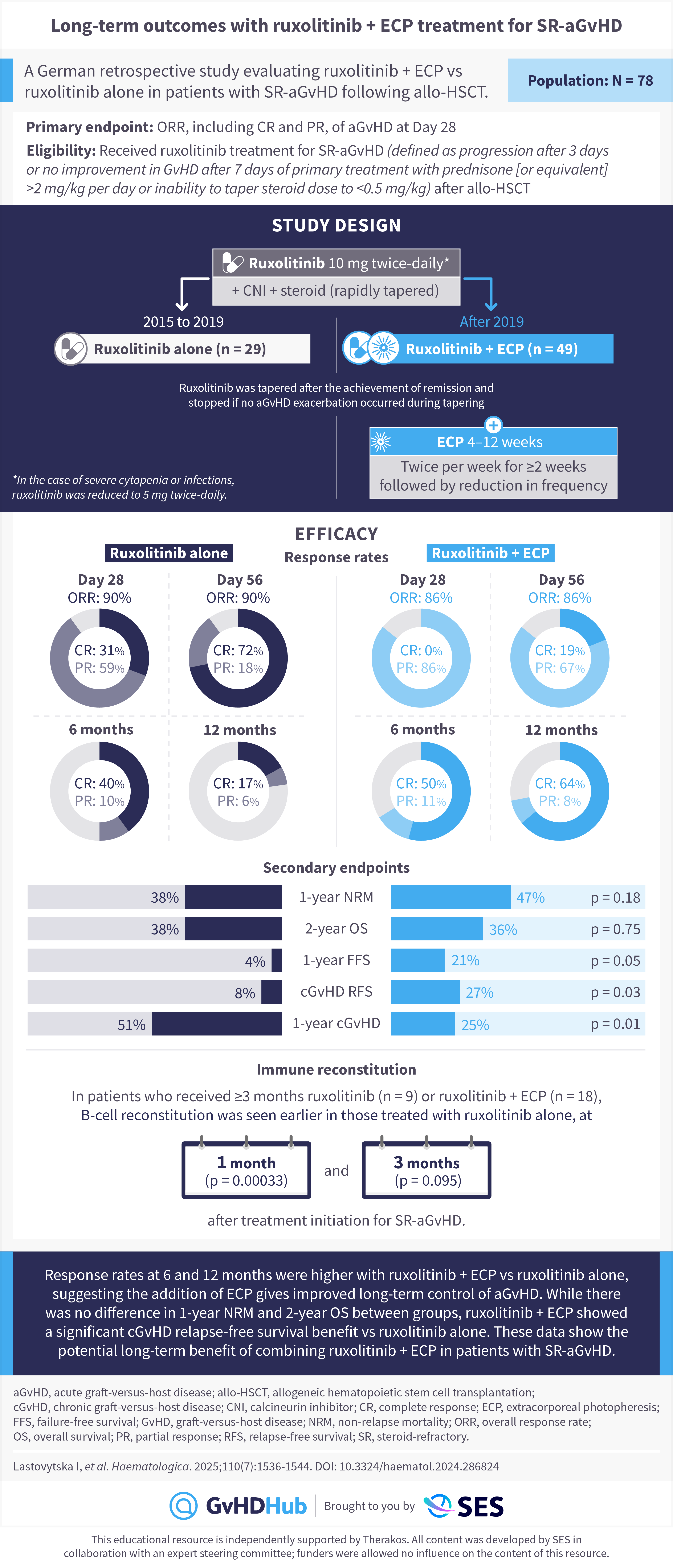
Limitations of this study include the retrospective nature, delay of ECP initiation in some patients (the median time between ruxolitinib and initiating ECP was 9 days), and imbalance of GvHD severity between the two treatment arms (Grade 4 SR-aGVHD was 45% in the ruxolitinib + ECP group vs 14% with ruxolitinib alone, p < 0.001). Despite this, combining ruxolitinib + ECP shows promise for the treatment of SR-aGvHD, with improved control of aGvHD and less cGvHD at one year compared with ruxolitinib alone.1
This educational resource is independently supported by Therakos. All content was developed by SES in collaboration with an expert steering committee; funders were allowed no influence on the content of this resource.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content

